
CT Angiography
Carotids, Aorta and more
Diagnostic Angiography: R.I.P.
Catheter based angiography is nowmuch less commonly performed fordiagnostic purposes.
More commonly used as part ofinterventional procedures.
Still useful when small vessels are thefocus.

Multidetector (Multislice) CTadvancing technology
Multiple axial images obtained pergantry rotation.
1989: single slice helical CT, 1 secgantry rotation
2004: 16 slice helical CT, 0.4 sec gantryrotation
2005: 32 and 64 slice scanners coming!
Non-invasive angiography
Non-invasive techniques are now thepreferred diagnostic studies in many cases
CTA or MRA
Multidetector CT makes studies very rapid andreliable
MRA can provide excellent images in patientswho cannot get IV contrast for CT, or in whomradiation exposure is an issue.
MRA has lightly less inherent resolution and issubject to artifacts from metal, blood flow.etc.
Advantages of noninvasiveangiography
Roadmap: enables planning of interventionalprocedure without diagnostic angiography
Shortens angiographic procedures
Enables infinite viewing angles
Angio much more limited
Can eliminate the need for conventionalangiography with negative study
Trauma
Dissection
Pre-op renal surgery
Renal artery stenosis
CT angiogrpahy – indications (2004)
Aorta
Carotid arteries
Circle of Willis
Renal arteries
Visceral vessels
Peripheral runoff
Coronary arteries?
CTA—technique
High contrast flow rates—needs at least 20gIV—need bright arterial enhancement
Thin sections to make 3D and reformattedimages more anatomic
High speed table movement to coveranatomy quickly during peak enhancement.
16 detector scanners have allowed the mostprogress in achieving the last two goals.
Thoracic CTA now takes about 8 seconds.
Arterialdensity
time
scan
Scan dynamics
Timing of scan is critical toimaging during peakarterial enhancement.
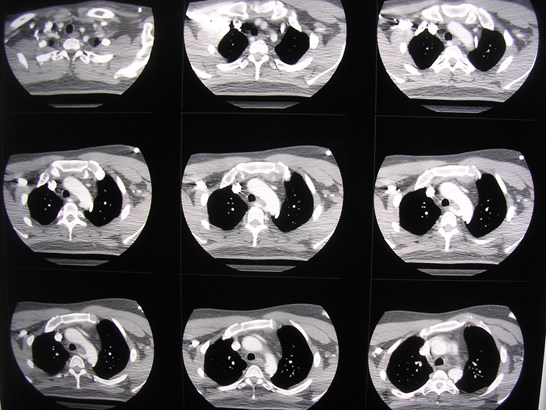
Lots of pictures!
Typical CTA of aorta is 300-400 images
Arterial runoff of legs is ~1200 images
Workstation viewing is essential for viewingaxial and multiplanar images.
Aorta—indications for CTA evaluation
Anomalies?
Aneurysm evaluation
Dissection?
Traumatic injury?
Penetrating ulcer?
Aberrant right subclavian artery
Angled AP view
Posterior view
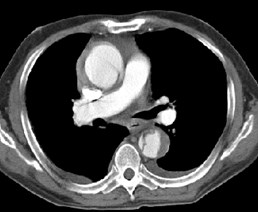
Aortic dissection
Intimal tear withhematoma orflowing blood in“false” lumen.
True and falselumina separatedby dissection flap.









True lumen
False lumen
Aortic dissection
Stanford type A: Flap involving ascending aorta(proximal to last great vessel) or great vesselsthemselves.
Usually needs urgent surgery
Risk of occlusion of great vessels or coronary arteries
Risk of aortic valve regurgitation or rupture intopericardium
Stanford type B: Flap only involves descending aorta
Usually medical management unless large branchvessel occlusion
Type A dissection



Dissection flap indescending aorta
Dissection flapin ascendingaorta
Dissection flap incarotid vessels
Type B dissection

Normalascendingaorta


True lumen
False lumen



Evaluate patency ofbranch vessels andtheir origins
Celiac axis fromfalse lumen
Right renal arteryfrom true lumen
79 year old with acute chest pain
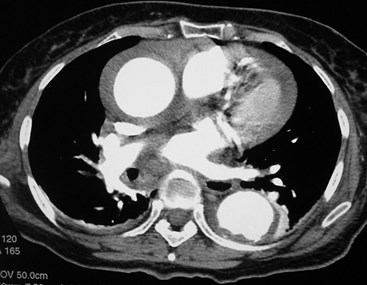


Reformatted images before and aftercontrast
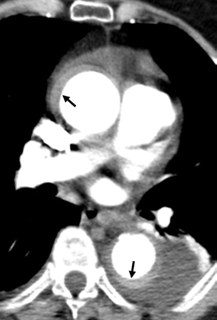
Aortic Intramural Hematoma
Bleeding into the medial layer of the aorticwall
No communication with the lumen
Originates from vaso vasorum
High density crescent in aortic wall
May see displaced intimal Ca++
Aortic Intramural Hematoma
Risk factors same as for acute aorticdissection
Symptoms same as for acute aortic dissection
Prognosis same as for acute aortic dissection
May be the precursor to acute aorticdissection!
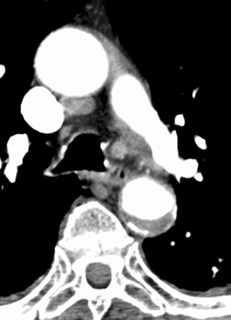
Best seen on non-enhanced scans:
Important to let radiologist know that scan is fordissection so that non-enhanced scans are done.
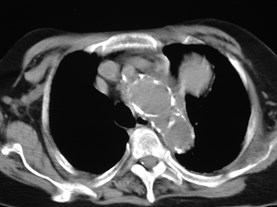
Aortic Intramural Hematoma

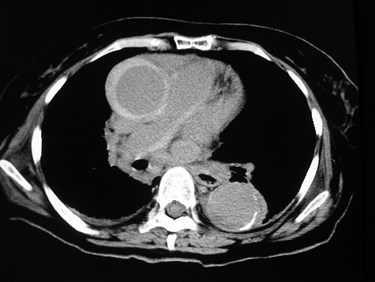
NOT!
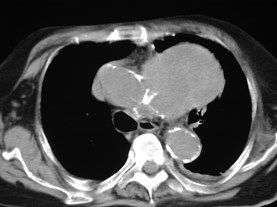
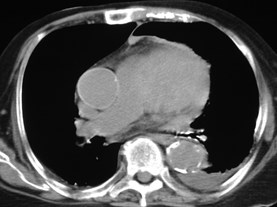
Mediastinal mass—biopsy?


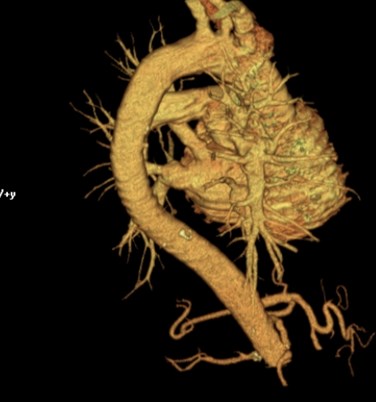
MRA: patient with chronic renalinsufficiency
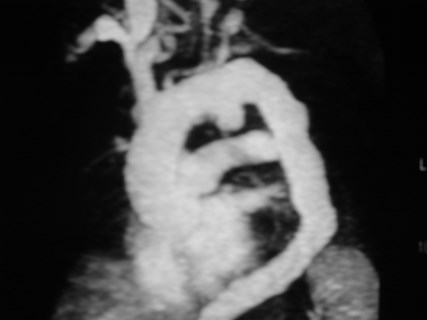
Large saccular aneursym,partially thrombosed
Motor vehicle accident:possible aortic injury

Normal aorta: no furtherevaluation is needed.
Mediastinal masses


Carotid artery
Importance of identifying patients whoare candidates for endarterectomy
Evaluation of carotids and vertebralarteries for other pathologies:
Fibromuscular dysplasia
Traumatic transection or dissection
Carotid artery
NASCET study
Endarterectomy beneficial in symptomaticpatients with >70% stenosis of ICA
Reduced risk of future stroke compared withmedical management
Possible benefit for patients with 50-69%stenosis
No relative benefit in <50% stenosis
Carotid artery
Doppler sonography as initial screening testfor ruling out carotid stenosis.
Limited in upper and intracranial ICA.
CTA findings equal to angiographic images
No risk of stroke as in angiography
4% TIA/minor stroke, 1% major stroke
Many surgeons now proceding on CT findings.
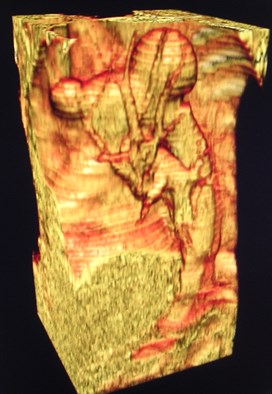
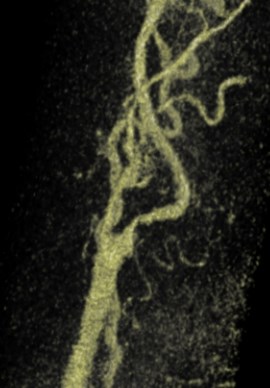
Normal carotid CTA
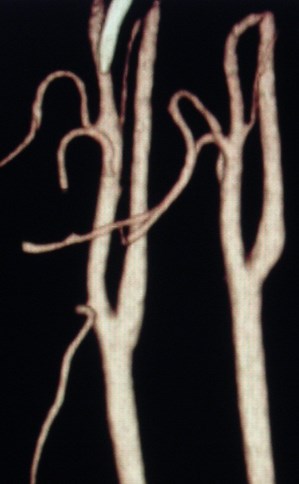
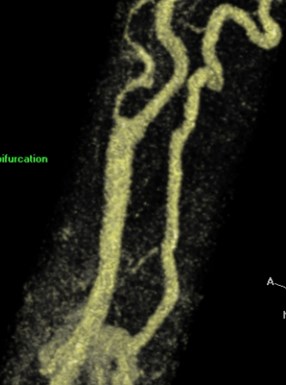
Critical carotid stenosis

TIA’s, abnormal carotid Dopplers


Measurementsto assessdegree ofstenosis
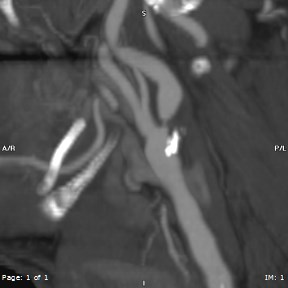
Ulcerated plaqueproximal ICA
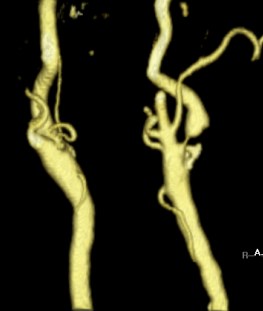
Asymptomatic carotid bruit
Narrowed R ECA
Narrowed L ICA
<50% stenosis of LICA
MRA
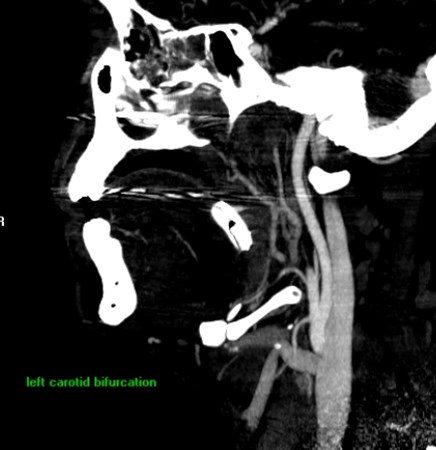
Gunshot wound to jaw

Carotid artery occluded
Stab wound to left neck
No injury to ICA ormajor ECAbranches
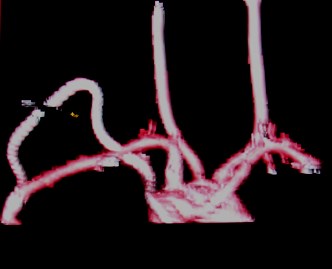
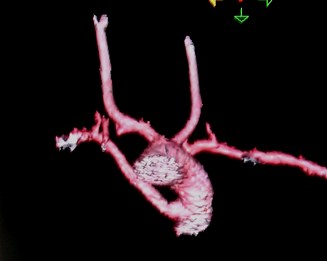
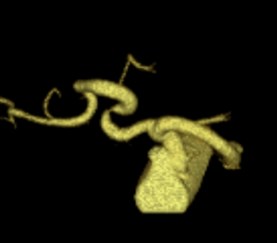
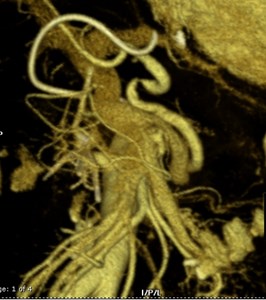
Circle of Willis intracranial vessels
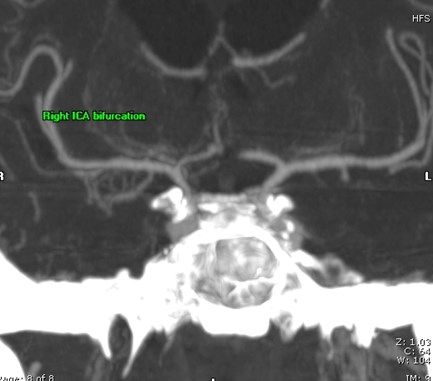
Circle of Willis—aneurysm search
Volume rendered images—any view youwant to display anatomy best


Visceral CTA—some indications
Abdominal aorta and larger branches
Aneurysm evaluation for size, interventionalplanning
Mesenteric artery evaluation for intestinalischemia
Vascular involvement by tumor?
Renal arteries for hypertension, donorevaluation
Chronic abdominal pain: ischemia?

Normal
Celiac and SMAnarrowing
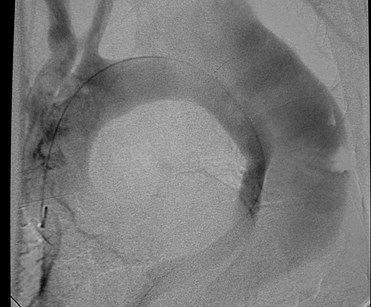
AAA stent-graft evaluation

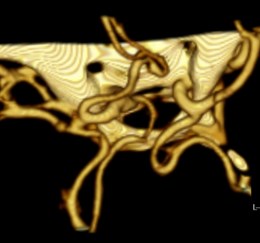
Living related donor evaluation
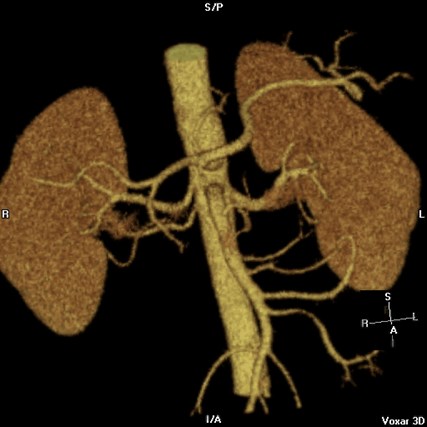
Duplicated right renal arteries
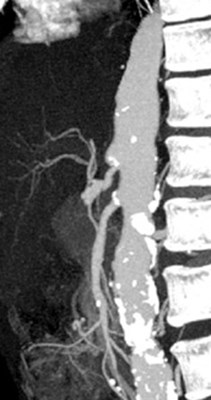
Hypertension—renal artery stenosis?
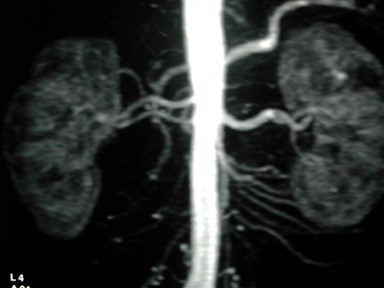
MRA—duplicated R renal artery,no narrowing.
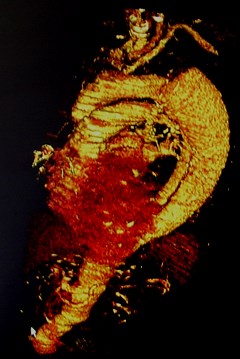
Aortic dissection—MRA
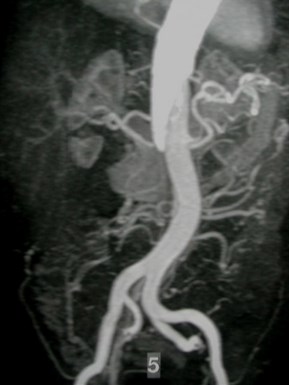
Bright contrast inslower flowingfalse lumen
AAA--MRA
Lumen well seenbut limitedevaluation ofthrombosed portionof aneurysm

One month post liver txp, rising LFT’s
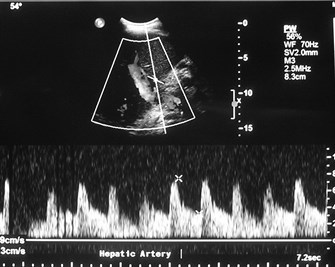
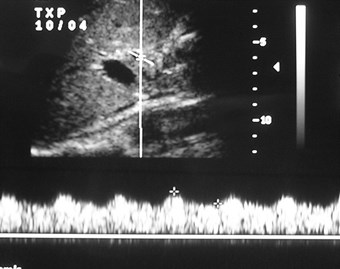
One month later
Just after transplant

Anastamotic stenosis of hepatic artery
Peripheral CTA--indications
Trauma
Ischemia
Tumors—preoperative roadmap
Thoracic outlet syndrome
Diminished radial pulse after trauma
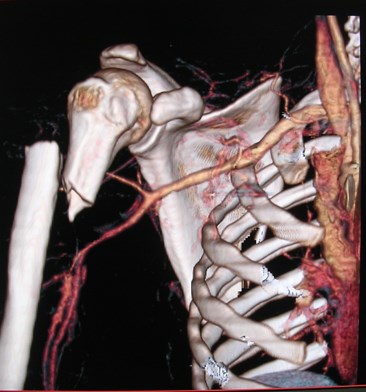
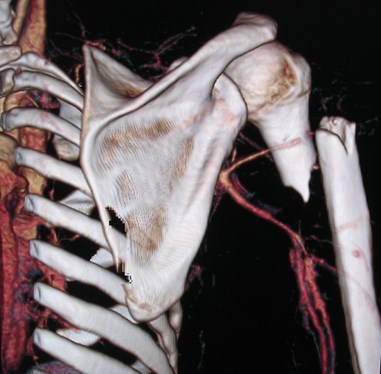
Normal axillary and brachial arteries
AP
PA
Right leg claudication


Tandem lesion ofR external iliacartery
Stent in Lexternal iliacartery
Pre-op for kidney transplant


Claudication
“runoff” study allowsevaluation of longsegments at once
Calcification showneasily
Long segmentobstruction of bothfemoral arteries

Coronary CTA
ECG-gated scans toreduce motion
16 or higher slicescanners
Aim to reduce numberof negative invasivecoronary angiograms

Multiplanar images
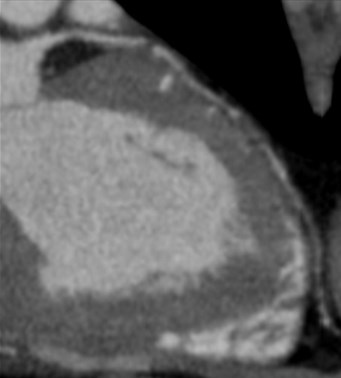
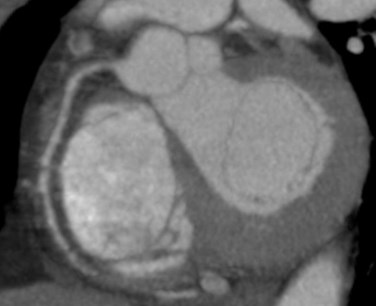
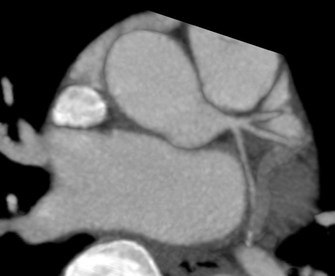
Normal RCA
Left main
Plaque andstenosis in LAD
Carotid CTA is indicated for all except:
A.Asymptomatic patient with carotid bruit
B.Patient with stroke after trauma
C.Patient with TIAs and Doppler US showingsevere stenosis
D.Patient with stab wound to lower neck
All are true except:
A.A negative thoracic aorta CTA is sufficient toend workup for thoracic aortic injury.
B.Thoracic CTA preferred to catheterangiography in evaluation of suspected aorticdissection.
C.Thoracic CTA can help in evaluation of aorticvalve insufficiency.
D.Intramural hematoma may be a precursor ofaortic dissection.
All are true except:
A.MRA is a good alternative to CTA in patientswith renal insufficiency
B.MRA resolution is equivalent to that of CTA
C.MRA allows multiplanar and volumerendered image formation
D.MRA images may be degraded by adjacentmetallic objects.
References
1.Barnett HJ et al Benefit of carotid endarterectomy in patients withsymptomatic moderate or severe stenosis. North American SymptomaticCarotid Endarterectomy Trial Collaborators.N Engl J Med. 1998 Nov 12;339(20):1415-25
2.Phillips CD et al CT angiography and MR angiography in the evaluation ofextracranial carotid vascular disease.Radiol Clin North Am. 2002 Jul;40(4):783-98.
3.Catalano C et al Infrarenal Aortic and Lower-Extremity Arterial Disease:Diagnostic Performance of Multi-Detector Row CT AngiographyRadiology 2004;231:555-563
4.Schoepf UJ et al CT of Coronary Artery DiseaseRadiology 2004; 232: 18-37.
5. Bruno Randoux et al Carotid Artery Stenosis: Prospective Comparison ofCT, Three-dimensional Gadolinium-enhanced MR, and ConventionalAngiography . Radiology. 2001;220:179-185.